In 2018, I attended the UNDP National Youth Parliament as a media corespondent. Young delegates from every state in the country came to participate…which brought to fore a predictable problem. Floor-time was largely spent on voicing grievances about the lack of translators. Delegates from the Hindi belt weren’t comfortable with English, while delegates from the Southern and North-Eastern regions weren’t comfortable with Hindi. I don’t remember what the conference agenda was because we barely got around to it.

It shouldn’t be groundbreaking to say that language is consequential to socio-political conversations, especially for already marginalized communities.
If progress and dialogue happening in one language cannot be effectively and promptly translated into other languages, some communities miss out where the rest of the world moves forward.
Self-Evident That All Dictionaries Are Created Equal
And yet some have slower developing scientific vocabularies. Why?
There are of course nuances to these broad, overarching factors. Some languages are actively excluded from both public and private projects. Especially if a language has only a few thousand speakers and even fewer readers, it is easily ignored in development efforts. There are also issues of access to Western science and/or the Internet, capital, issues of geography, literacy, caste…the list goes on.
These varied factors become most evident when observing individual cases, while the two overarching factors remain largely constant. Regardless, the effect remains — the concerned community is excluded from the fruits of scientific progress.
And nowhere is this most directly fatal than in the healthcare space.
ओर्गास्म, पी.सी.ओ.डी, फैलोपियन ट्यूब…
I learnt this at college while conducting sessions on puberty and menstruation for the campus housekeeping staff. I created a Hindi script for the menstrual cup demonstrations I was to conduct, avoiding technical English terms as far as possible to ensure the language was accessible to my didis, who primarily spoke Haryaanvi.

I realised that while there were Hindi equivalents to the organs and conditions I needed to refer to, they were of a more Sanskritised Hindi bent than the Urdu-Hinglish that is colloquially spoken. Moreover, I found these words only in dictionaries and no one from my audience recognized them. So while the vocabulary does technically exist, it is obscure and inaccessible.
Wherever there were no everyday Hindi terms to pick from, my didis would ask to write down the English terms in devnagari, committing them to memory. Those who couldn’t write simply slid past the technicality and used ‘वो’ as a placeholder.
“वो उसके अंदर जाता है तो वो होता है. When ‘that’ goes into ‘that’, ‘this’ happens.”
It was clear to me from these interactions that not only were conversations about reproductive health in this Haryaanvi-speaking community non-specific but also schools, acquaintances, and medical professionals had failed to allow the community’s women the vocabulary to understand their own bodies.
And this is the first level at which ignoring regional languages compromises healthcare:
‘Disabled’ is not পাগল, മന്ദബുദ്ധി, பைத்தியம்…
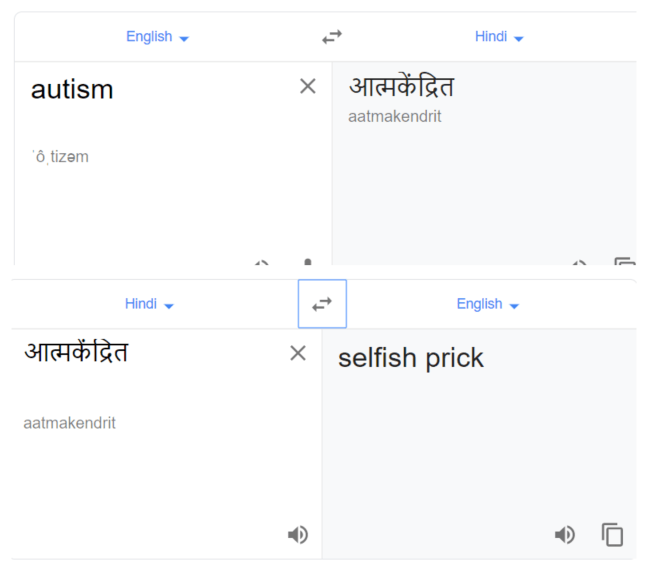
While working in the disability healthcare space, I once asked my peers to send me words in their languages that referred to people with IDDs. I wanted to understand how many terms spoken colloquially are technical names for disabilities and how many are in fact derogatory slurs.
Unsurprisingly, the vast majority of the responses I received translated roughly to ‘crazy, ‘retarded’, or at the least ‘slow’.
My cousin has what’s called ‘Down Syndrome’. I have never heard those two words come from the mouth of anyone in my family. I’m a native Gujarati speaker and those who taught me the language cannot tell me the formal equivalent for ‘intellectual disability’.
In colloquial conversation, we skirt around stigmatised disorders to the extent that learning the formal terminology becomes unnecessary.
“એને મગજ માં કઈ થયું છે” or ‘Something (problematic) has happened to their brain.’ is the typical Gujarati equivalent for all Intellectual and Developmental Disabilities (IDDs). There is no distinction between Autism, Down Syndrome, Global Developmental Delay, or other sub-categories of IDDs. Hence regardless of very fundamental differences in their conditions, Gujarati speakers by default relegate anyone with an IDD to a single “abnormal” out-group.
And this is the next level at which ignoring regional languages compromises justice:
Vague Diagnosis, No Prognosis
This phenomenon — of slurs replacing formal diagnoses — is not restricted to casual co. Medical professionals may also find themselves using these terms in the absence of more specific and sensitive vocabulary.
I remember a conversation with my co-worker about a renowned psychiatrist in Hyderabad. It had come to fore that upon assessing a child with Autism Spectrum Disorder, he had refrained from giving the child’s non-English-speaking parents a named diagnosis. Rather, he simply said “आपका बेटा पागल है. Your child is mad.”
When confronted by my colleague, he said, “इन लोगों को बोलने से क्या फायदा? What’s the use of giving details to such people?” This is the real-world impact of the classist bias against non-English languages— a doctor not bothering to afford his patient a diagnosis on the assumption that non-English speaking parents wouldn’t understand the complexities of the their child’s condition.
I wonder if a lack of practice of translating English medical language to regional languages contributed to his inhumane forfeiture of duty.
And this is the next level at which ignoring regional languages compromises healthcare:
And this is far from an isolated incident…
Case Study: Can’t Throw Money At It
To maintain anonymity, this case study is about one SchoolX in AreaX of coastal Andhra. It is blessed with foreign aid, state-of-the-art infrastructure, and a vast campus. What’s even more comforting is that the founders and staff display a genuine zeal to do right by their students.
Students here have physical, developmental, and/or intellectual disabilities (IDDs), and SchoolX invited our organisation to conduct a workshop for their parents. My colleagues left prepared for an advanced session. They collaborated with an expert from another organisation in Bangalore, and took off for AreaX from Hyderabad.
When they reached the campus and interacted with the staff, they realised that the session they had planned would not do. It turned out most of the school’s staff themselves had little basic understanding of the different IDDs. Before an advanced session, an extremely rudimentary session on the medical basics of disabilities was imperative.
Now of course this unfortunate situation is a product of a multitude of factors:
- Geography AreaX is isolated. The closest clinics and doctors with assessment facilities are hard to reach. Not too many experts drop by.
- Income This is a rurality and labour is largely manual. For parents, a trip to a city doctor means losing a day’s work, plus the travel costs in addition to medical fees. The result is that few children have a diagnosis and fewer still have an accurate diagnosis.
- Literacy Since AreaX is a rurality, the quality of education leaves much wanting. Thus, parents have few means to inform themselves better about their child’s condition and access to online resources becomes meaningless.
And these factors were only exacerbated by the fact that most parents only spoke Telugu.
Parents had sparse and often inaccurate information about their children’s conditions. Many were simply labeled ‘Mentally Retarded’ despite their symptoms almost if not certainly indicating Autism Spectrum Disorder or Down Syndrome. Without accurate diagnoses, it is no wonder the families were unable to identify which care and therapies were necessary!
My colleagues got to work, meeting each family separately to detail for them their child’s disorder, the challenges that would come with, and the therapies required. “Parents wrote down every word”, my colleague told me, “making sure they got down in black and white all the correct English spellings, since they had no frame of reference in Telugu.” To recap:
So? Now what?
Building vocabularies is not a one-time gig. This is not the agenda for a 3-year task-force with absolute authority. It’s a semi-organic continual process, involving interaction among the whole language community. It never concludes, only speeds up or slows down.
And speeding it up is crucial. Inequalities of language exacerbate inequalities of access. Sparse healthcare understanding is heavy especially on women, PWDs, and senior citizens.
Making medical discussions accessible is not pedantic nit-picking. It is affording marginalized peoples the right to wholly understand and make informed choices about their bodies.
For the moment, I’m waiting for someone to give me a phrase to take to my naani so she can finally describe her grandson with dignity…



0 Comments